📞 +44 0161 495 7011 (9am - 5pm ᐧ Mon - Fri)
Testicular cancer is a condition where malignant cells develop in the tissues of one or both testicles. These oval-shaped organs, housed within the scrotum, are responsible for producing sperm and the primary male sex hormone, testosterone. While it is relatively rare compared to other urological conditions, it remains the most common cancer affecting men between the ages of 15 and 49 in the UK.
The disease typically begins in the germ cells, which are the cells responsible for creating sperm. Most cases are highly treatable and curable, especially when identified in the early stages. However, because it often affects younger men who may not be accustomed to regular health screenings, awareness and prompt action are vital.
Relevant Fact:
In the United Kingdom, approximately 2,400 new cases of testicular cancer are diagnosed every year. Despite this, it has one of the highest survival rates of any cancer, with more than 96% of men surviving for 10 years or more after diagnosis.
Symptoms
The most common sign of testicular cancer is a painless lump or swelling. However, several other indicators should prompt a consultation:
- A Palpable Lump: A small, hard lump, often described as feeling like a pea or a grain of rice, located on the front or side of the testicle.
- Changes in Texture: A testicle that feels unusually firm, hard, or has changed its regular consistency.
- Heaviness: A dragging sensation or a feeling of increased weight in the scrotum.
- Size Discrepancy: While it is normal for one testicle to be slightly larger or hang lower than the other, a significant or sudden change in size should be noted.
- Ache or Discomfort: A dull ache in the lower abdomen or the groin area.
- Late Stage Signs: If the cancer spreads to the lymph nodes or lungs, symptoms may include back pain, a persistent cough, or shortness of breath.
Mr Collins Approach
Having conducted MD research at the Mayo Clinic and Edinburgh University, Mr Collins focuses on what is clinically significant for the individual. This means carefully staging the disease and discussing the nuances of treatment, such as the timing of surgery and the preservation of long-term health, rather than rushing a generic plan. His role as the European Editor of The Prostate Journal at Harvard ensures that his practice is always at the forefront of global oncological research.
Causes & Risk Factors
While the exact cause of testicular cancer remains unknown, several factors are known to increase a man’s risk:
The Solution: Treatment pathways
The primary objective of treatment is to remove the cancer while preserving quality of life and future fertility.
Surgical Intervention:
The standard treatment is an orchidectomy, which is the surgical removal of the affected testicle. This is usually performed through an incision in the groin. To address the aesthetic and psychological impact, Mr Collins offers the option of a prosthetic (artificial) testicle, which can be inserted during the same procedure to maintain a natural appearance.
Medical Management:
Following surgery, the removed tissue is analysed to determine if it is a seminoma or a non-seminoma. Depending on the stage and type:
- Surveillance: For low-risk cases, regular scans and blood tests are used to monitor the patient without further immediate treatment.
- Chemotherapy: Used to kill any remaining cancer cells and reduce the risk of recurrence.
- Radiotherapy: Often used for seminomas that have spread to the lymph nodes.
Fertility Preservation:
Because treatments can affect sperm production, Mr Collins ensures that “Sperm Banking” is discussed and arranged before any intensive treatment begins, providing peace of mind for future family planning.
How to Prevent?
There is no known way to prevent testicular cancer, as it is not linked to lifestyle choices like smoking or diet. Therefore, the focus is entirely on early detection through self-examination.
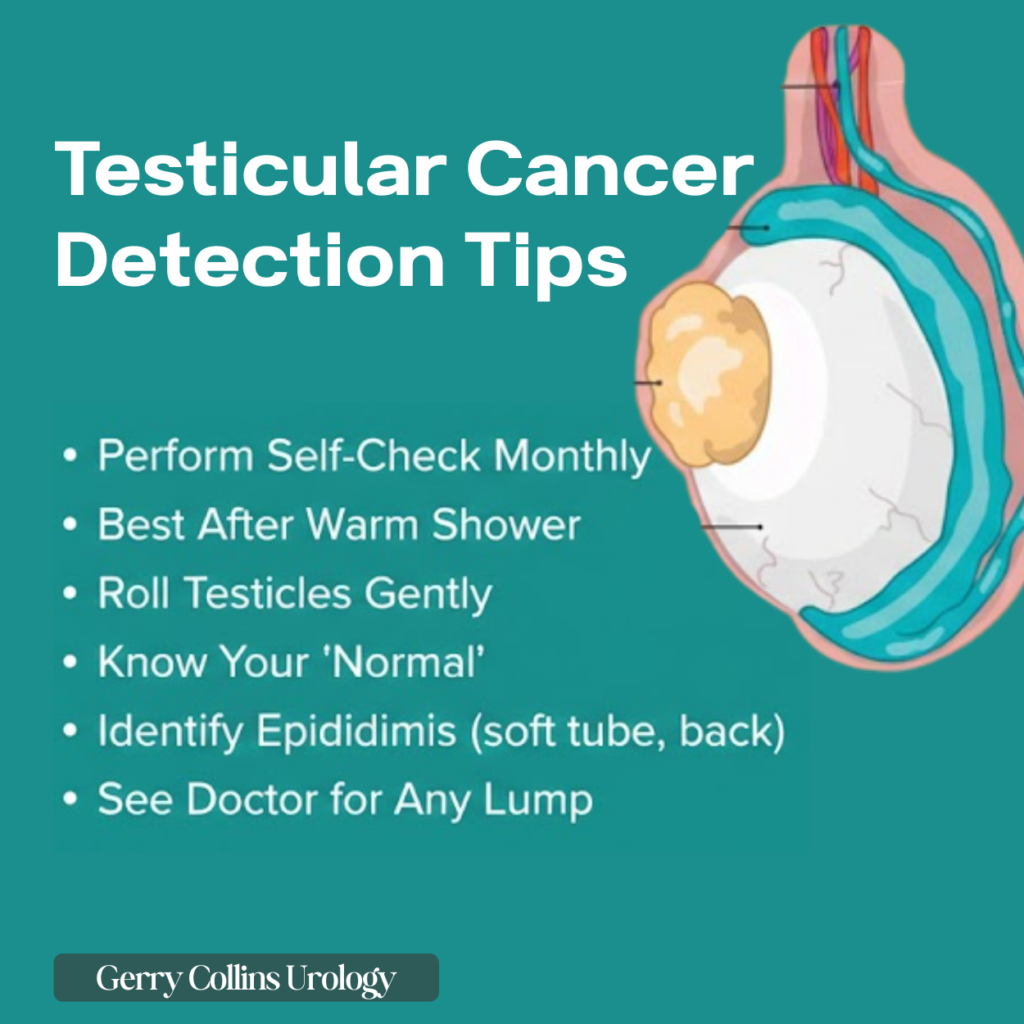
- The Monthly Check: You should examine your testicles once a month.
- The Best Time: Perform the check after a warm bath or shower. The heat relaxes the scrotum, making it much easier to feel for anything unusual.
- The Technique: Use both hands to roll each testicle between your thumb and fingers. Get to know what is “normal” for you.
- Identify the Epididymis: Do not be alarmed by a soft, coiled tube at the back of the testicle. This is the epididymis, which stores sperm, and it is a normal part of your anatomy.
- Act Quickly: If you find a lump, do not wait for it to go away. Most lumps are benign cysts or swollen veins (varicoceles), but only a specialist can provide the certainty required.
FAQs
Will I still be able to have sex and get erections?
Yes. Removing one testicle does not typically affect your ability to have an erection or perform sexually. The remaining healthy testicle usually produces enough testosterone to compensate.
Will it affect my ability to have children?
Having one testicle removed generally does not cause infertility, as the remaining one continues to produce sperm. However, if chemotherapy or radiotherapy is required, fertility can be affected. This is why we prioritise sperm banking before these treatments begin.
Is the surgery painful?
The procedure is performed under general anaesthesia. Post-operative discomfort is usually well managed with standard pain relief, and most men return to light activities within a week or two.
Is it definitely cancer if I find a lump?
No. In fact, most lumps found in the scrotum are not cancerous. They are often harmless cysts or fluid collections. However, because you cannot tell
Based in Manchester and Cheshire, Mr Gerald Collins is currently accepting private consultations for the assessment of kidney masses, haematuria, and general urological concerns. With 29 years of experience, he provides the clarity and expertise needed to move from uncertainty to a confident treatment plan.


