📞 +44 0161 495 7011 (9am - 5pm ᐧ Mon - Fri)
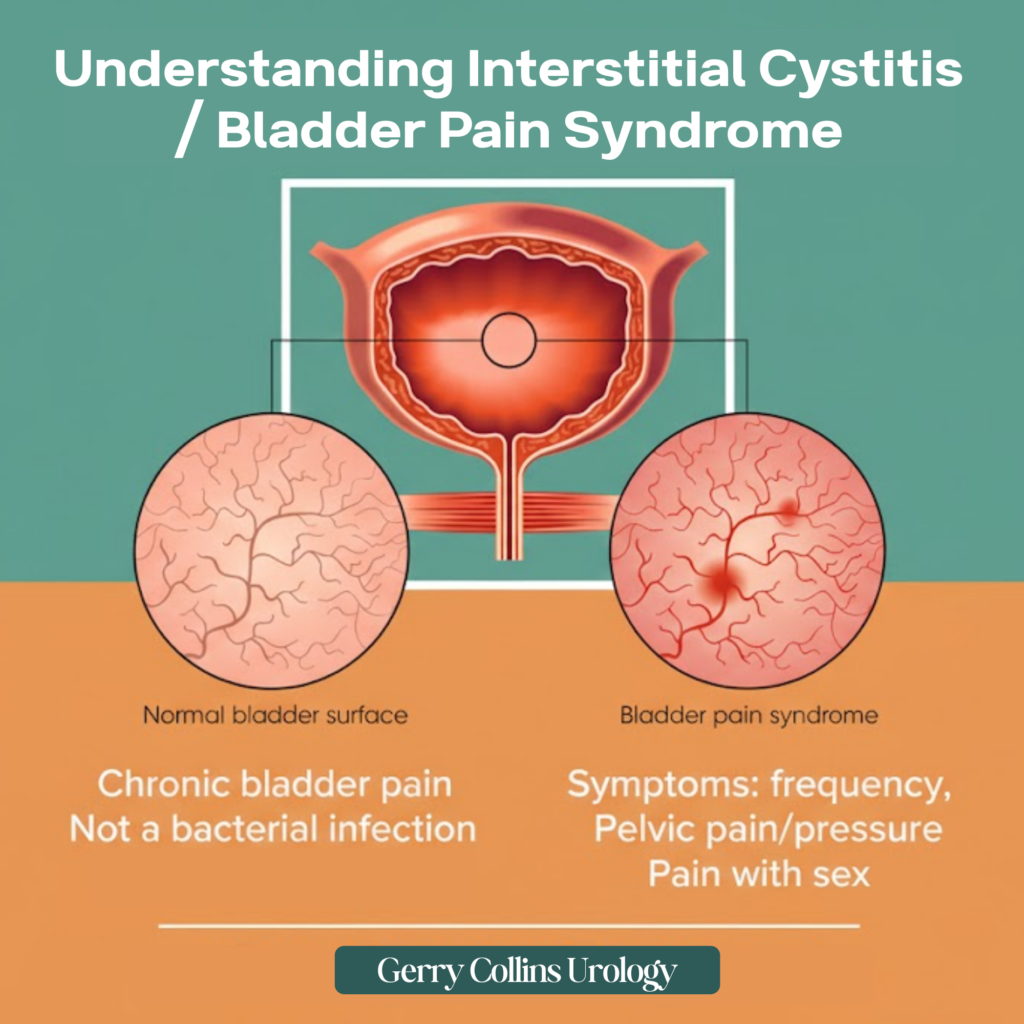
Interstitial Cystitis (IC), increasingly referred to as Bladder Pain Syndrome (BPS), is a chronic, often debilitating condition characterised by recurring pain or discomfort in the bladder and the surrounding pelvic region. Unlike a standard urinary tract infection (UTI), BPS is not typically caused by bacteria, meaning antibiotics rarely provide lasting relief. Instead, the inner lining of the bladder becomes irritated, inflamed, or sensitive, leading to a cycle of urgency and discomfort.
For many, the condition manifests as a persistent need to pass urine, often in small amounts, alongside a heavy, aching pressure in the lower tummy or pelvis. While it is more common in women, it significantly affects men as well, often being misdiagnosed as chronic prostatitis. Though there is currently no universal cure, the focus of modern urology is on strategic management: identifying unique triggers and cooling the “biological fire” within the bladder wall.
Symptoms
Because BPS symptoms can mimic other conditions, it is vital to recognise when your symptoms require specialist investigation. You should seek a consultation if you experience:
- Persistent pain in the bladder, lower tummy, or pelvic floor that does not resolve with standard treatments.
- An overwhelming and frequent urge to urinate, even when the bladder is empty.
- Nocturia: Waking up multiple times during the night to pass urine.
- Pain during or after sexual intercourse (penetration for women) or pain during erection or after ejaculation for men.
- Visible blood in the urine (haematuria): This requires urgent assessment to rule out other underlying causes.
- Symptoms that “flare” or worsen in response to specific triggers like stress, certain foods, or the menstrual cycle.
Mr. Collins Approach
With nearly 30 years of experience and a background in rigorous research at Edinburgh University and the Mayo Clinic, he understands that for a patient in pain, the “wait and see” approach only breeds anxiety.
In men, he carefully distinguishes BPS from BPH (enlarged prostate) or prostatitis, ensuring patients are not subjected to unnecessary treatments. By viewing every diagnosis through the lens of neovascularity and bladder biology, he filters out the clinical noise to create a highly personalised, measured intervention plan that respects the patient’s individual baseline.
Causes & Risk Factors
While the exact cause of BPS remains a subject of ongoing research, several factors are believed to contribute to the irritation of the bladder wall:
Treatment pathways
Mr Collins focuses on a tiered approach, starting with the least invasive options and progressing to more advanced therapies where necessary.
Medical & Therapeutic Pathways:
- Oral Medications: This includes everyday painkillers, antihistamines to reduce inflammation, or nerve-blockers like amitriptyline to dampen pain signals.
- Bladder Instillations: Often called a “bladder cocktail,” this involves delivering soothing medicine (such as sodium hyaluronate or heparin) directly into the bladder via a thin catheter to protect the lining.
- Neuromodulation: Sacral nerve stimulation (SNS) involves a small device that sends electrical signals to the nerves controlling the bladder, helping to reset the “urgency” signals.
- Specialist Pelvic Physiotherapy: Targeted exercises to relax and coordinate pelvic floor muscles, which are often in a state of chronic spasm in BPS patients.
Surgical & Advanced Pathways:
- Cystoscopy with Bladder Overdistention: A procedure to stretch the bladder under general anaesthetic, which can sometimes desensitise the nerves and improve capacity.
- Resection of Hunner’s Ulcers: If specific lesions (ulcers) are found on the bladder wall, they can be cauterised or removed using a laser.
- Major Surgery: In extreme cases where all other treatments have failed, options such as a reconstructed bladder (neo-bladder) or urinary diversion may be discussed.
How to Prevent?
Managing BPS often starts with proactive changes at home to reduce the frequency of flare-ups:
- The Food Diary: Track your intake to identify personal “triggers.” Common culprits include caffeine, alcohol, spicy foods, and highly acidic items like citrus fruits and tomatoes.
- Bladder Retraining: Gradually increasing the time between bathroom visits can help the bladder learn to hold more urine over time.
- Stress Management: Stress is a known trigger for pelvic pain. Incorporating low-impact exercise like yoga or meditation can help regulate the nervous system.
- Smoking Cessation: Smoking irritates the bladder and restricts blood flow, hindering the natural healing process of the bladder lining.
FAQs
Is Interstitial Cystitis just a permanent urine infection?
No. While the symptoms are similar, IC/BPS is usually a sterile condition, meaning there is no active bacterial infection. This is why standard antibiotics often fail to work.
Can men get Bladder Pain Syndrome?
Yes. In men, BPS is frequently misdiagnosed as chronic prostatitis because the symptoms of pelvic pain and urinary frequency overlap. A specialist urological assessment is necessary to distinguish between the two.
What is the Stockholm3 test’s role here?
While the Stockholm3 test is primarily an advanced tool for prostate cancer risk assessment, Mr. Collins utilises such high-level diagnostics to “rule out” malignancy in male patients presenting with bladder pain, ensuring that the diagnosis of BPS is accurate and not masking another condition.
Will I have this pain forever?
While BPS is a long-term condition, most patients find significant relief through a combination of lifestyle changes, medication, and clinical interventions. The goal is to move from “crisis management” to long-term stability.